

Is It Appropriate To Treat Medical Care As A Commodity Like Other Goods And Services
AHA! Healthcare Is Both a Right and a Commodity
In tardily January, I participated in an Oxford-fashion fence regarding whether healthcare is a commodity. The debate was the featured outcome at Tata Memorial Centre's Platinum Jubilee Conference in Bombay, Republic of india.
A packed auditorium of over a thousand attendees buzzed with excitement as Professor Antonio "Tito" Fojo (my opponent) and I walked on-stage. The conference theme, "HEALTHCARE: A Commodity or Basic Human Need?" put the spotlight on our contest. We were midway through the iii-day conference, and it was show-fourth dimension.
Dr. Benjamin Anderson moderated our debate. Dr. Anderson is a respected global health leader and currently chairs The Breast Health Global Initiative at the Fred Hutchinson Cancer Enquiry Center in Seattle, Washington. Ben, Tito and I became fast friends as nosotros prepared for the debate.
My role was to argue in favor of the motion that healthcare is a commodity. Tito is a world-renown cancer researcher and gifted public speaker. As we waited for introductions, he whispered that I had "drawn the short straw." Tito was more right than he could have imagined.
Ben conducted the pre-debate vote. Only 3 audition members agreed with the proposition that healthcare is a article. In overwhelming numbers, the audience asserted that healthcare is a basic human need and right. Stepping up to the podium, I clearly had some explaining to do.
Rhetoric and Reality
Ironically, making healthcare a right doesn't interpret into universal healthcare access. Far from it. In rich and poor counties alike, societies struggle to provide appropriate intendance at appropriate prices. The The states spends far more than per-capita on health expenditure than any other country, merely has pregnant over-utilization along with sizable coverage and access gaps.
At the other end of the economic spectrum, the Indian Constitution proclaims healthcare is a basic human right for its citizens. Despite this, Bharat has enormous unmet medical needs and limited insurance coverage. 70% of Indian healthcare transactions occur on a cash "pay every bit you go" basis.
Throughout the earth, societies provide and pay for healthcare services. Their healthcare policy debates center on the advisable office for government in service delivery, payment, guaranteeing access and regulating market participants.
No national health organization is perfect. All struggle to manage need for healthcare services, provide equitable access and control costs. Absent transformation, healthcare will swallow disproportionate amounts of national resources in all countries without commensurate increases in national wealth.
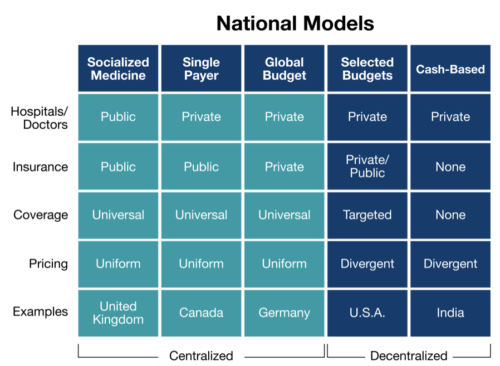
The chart below summarizes the five different models that nations use to distribute healthcare services. These models are wide categorizations. Within countries, health systems showroom nuanced differences and may incorporate features from multiple models.
The Healthcare Anomaly
Scottish philosopher and economist Adam Smith published The Wealth of Nations in 1776. In his treatise, Smith explained how the market's "invisible mitt" allocates resources more efficiently and thereby creates wealth. Smith'southward theories created the conceptual foundation for modern capitalism.
As Smith prophesized, de-centralized complimentary-market systems consistently outperform centrally-planned economic systems. Backer economies classify resources more than effectively and more than efficiently than market socialist economies. Capitalism's higher productivity generates disproportionate national wealth. Capitalist South korea's economic prosperity dwarfs that of socialist North korea.
While capitalism has thrived in the manufacturing, wholesaling and retailing sectors, information technology has under-performed in healthcare. To date, centralized systems have generated superior health status for lower costs than decentralized systems. Does this mean that the healthcare industry is fundamentally different than other industries and operates outside the boundaries of established economic theory?
The consequences of market failure in healthcare can lead to serious injury or even death. With stakes this high, nigh advanced economies centrally plan, toll and regulate healthcare services. Examples include socialized medicine (Bully U.k.), single-payer systems (Canada) and global healthcare budgeting (Germany).
Centralized systems coordinate healthcare service provision and payment. Prices are uniform and coverage extends to all citizens. Implicit in this preference for centrally-administered healthcare is the conventionalities that highly-regulated, regime-led healthcare delivery is more reliable and efficient than free-market place approaches.
Proponents of centrally-administered health systems argue that healthcare differs from other businesses in the following important ways:
- Buyers and sellers of healthcare services do non have complete (and perfect) data when executing transactions, and then they cannot brand meaningful judgements regarding the quantity, prices and relative benefits of specific healthcare products.
- The being of "externalities" (due east.thou. the costs of grooming doctors) expands the benefits and costs of healthcare transactions beyond buyers and sellers.
- Uncertainty related to healthcare symptoms, handling and outcomes complicates service pricing. Stomach pain could result from indigestion or a cancerous tumor.
- Adverse selection in the purchasing of healthcare insurance distorts market place participation. Those who require healthcare services disproportionately purchase health insurance coverage.
- A small percentage of the population consumes a disproportionate share of healthcare expenses. In the U.s.a., for, case, v% of patients eat 50% of total wellness expenditures.
- Moral hazard and "free-riding" in receiving healthcare services wastes resources. Many patients consume far more healthcare services than they require, especially when third-parties pay for the consumed services.
- In that location is significant information asymmetry. Doctors and caregivers know more than patients, which can lead to passive acceptance of medical recommendations or unrealistic distrust.
- Perverse fiscal incentives stimulate over- and nether-treatment.
- Those who cannot pay for healthcare services forgo necessary treatments.
- Monopolistic/predatory pricing tin occur when vital healthcare products (due east.g. drugs) and services are in scarce supply.
There are examples of healthcare services (e.yard. ophthalmology) with transparent pricing and great customer service. It's easy and affordable to get middle check-ups and buy glasses, even on nights and weekends. Such services are the exception; however, non the rule.
From all apparent evidence, it seems reasonable to deduce that centralized systems allocate scarce healthcare resources more than efficiently and effectively than de-centralized health systems. Deductive logic is powerful, only non e'er accurate.
The flaws in healthcare markets identified above are real, but likewise exist in other markets to greater and bottom degrees. Economists utilize regulation to mitigate these flaws, residuum supply-demand relationships and create level competition.

There'south Danger in Deductive Reasoning
Another Scottish philosopher from the 1700s, David Hume, found fault with "if-then" deductive reasoning. Hume believed in the power of data-driven inductive reasoning and used just-discovered blackness swans to illustrate his logic.
That there were no recorded sightings of black swans, Hume observed, did not negate their existence. To the contrary, the sighting of only i black swan proved that not all swans were white.
As the penguin cartoon illustrates, flawed logic tin can to pb to flawed conclusions. While healthcare markets are complex, they exercise not operate outside the laws of economics and human being beliefs.
Applying Hume's inductive reasoning to national healthcare systems, we cannot conclude that centralized healthcare systems will e'er outperform de-centralized health systems. Given advisable market structure and incentives, de-centralized markets for healthcare services perform exceeding well.
Consider how the cost and quality of healthcare services can alter when exposed to marketplace forces. Many procedures that once epitomized specialty care, such as articulation replacement surgeries, have become commonplace. Consumers tin now "shop" for the best service providers. With increased transparency, procedure prices driblet and quality, service and client experience improve.
Routine healthcare services that exhibit broad pricing variation today are actually commodities and should price accordingly. MRIs, joint replacement surgeries and other high-volume, low-run a risk procedures are essentially retail products. When unleashed, American consumers are value-seeking machines. Market-based reform efforts eye on giving purchasers sufficient information to buy healthcare services more than wisely.

The Business of Healthcare
If healthcare is a basic right, it besides is a business organization. Market participants respond to economical incentives, allocate resource, brand investments and generate returns. While the de-centralized healthcare systems in the United states and Republic of india have under-performed their peers to engagement, they likewise are the engines of innovation transforming healthcare commitment.
Republic of india's cash-based healthcare delivery model means admission to health services is largely a role of cost. Unmet demand for vital surgeries is loftier. The lower the surgical price, the more Indian people can afford surgery. In response to this market reality, "focused surgical factories applying advanced manufacturing principles have emerged to comport high-volume, loftier quality surgeries at a fraction of the U.South. cost.
In the U.Southward., unprecedented levels of private equity and venture investment are funding innovative healthcare companies that are attacking the system'south embedded inefficiencies. They volition win in the healthcare marketplace by delivering superior outcomes at lower prices with greater client convenience.

Dorsum to Mumbai: AHA Moments!
Ben, Tito and I concord that healthcare is both a right and a commodity. Ben generously offered this alternative to audition members upon conclusion of the contend. Two-thirds voted in favor of this proposition. We all declared victory! This was an "AHA moment."
People deserve Advisable, Holistic and Affordable healthcare services that are Coordinated, Accessible, Reliable and Evidenced-based. This is AHA Intendance! A better debate question is whether centralized or decentralized healthcare systems can meliorate evangelize AHA CARE!
Harvard Professor Amitabh Chandra observes that "Americans pay Ferrari prices for Camry healthcare services." He'southward correct. Hard-working Americans deserve better. Healthcare's claiming is to deliver on the hope of marketplace-driven transformation, so that all Americans can receive the right care at the right time in the right place at the right price.
Healthcare reform is our generation's most compelling public policy challenge. American ingenuity is finding ways to evangelize better healthcare services for less coin. This will unleash enormous resource to pay higher wages and make investments in more productive industries. In the process, America's de-centralized healthcare organization will leapfrog centralized national health systems in all relevant metrics.
Outcomes thing. Customers count. Value rules. Somewhere in Scotland, Adam Smith and David Hume are smiling.

Is It Appropriate To Treat Medical Care As A Commodity Like Other Goods And Services,
Source: https://www.4sighthealth.com/aha-healthcare-right-commodity/
Posted by: fishervered1989.blogspot.com
0 Response to "Is It Appropriate To Treat Medical Care As A Commodity Like Other Goods And Services"
Post a Comment